Glenohumeral Joint Dislocation on Chest X-ray: A Radiologic Perspective
Glenohumeral Joint Dislocation on Chest X-ray: A Radiologic Perspective
Abstract
Glenohumeral dislocation, the most common type of joint dislocation in the human body, is frequently encountered in emergency and orthopedic settings. Although shoulder radiography is the gold standard, chest radiography (CXR) may incidentally capture dislocations and should not be overlooked, particularly in trauma contexts.
Introduction
Shoulder dislocation is a frequent orthopedic emergency, with anterior glenohumeral dislocations accounting for 95% of all shoulder dislocations. While dedicated shoulder views such as the AP, axillary, and scapular Y views are standard for assessment, incidental findings on chest radiography can offer critical diagnostic clues, especially in trauma evaluations where a chest X-ray may precede targeted imaging.
In this column, we analyze a classic case of anterior shoulder dislocation visible on a chest X-ray, delve into the radiologic interpretation, and provide clinical context, relevant anatomy, and management implications.
Figure 1: Radiological Example
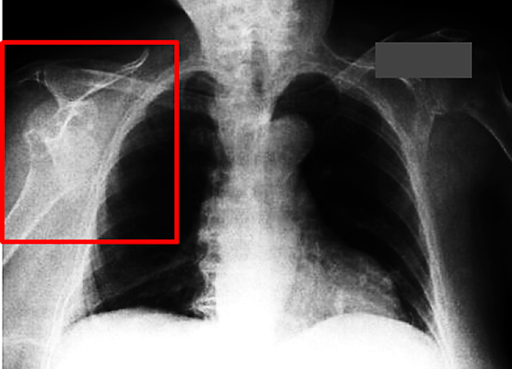
Figure 1. Chest X-ray demonstrating right anterior glenohumeral dislocation. The humeral head is displaced inferiorly and medially, no longer articulating with the glenoid fossa.
Radiologic Anatomy of the Shoulder
The glenohumeral joint is a ball-and-socket articulation between the humeral head and the glenoid cavity of the scapula. It allows the greatest range of motion of any joint, but at the expense of stability. The primary stabilizing structures include:
-
Glenoid labrum
-
Rotator cuff muscles (SITS: supraspinatus, infraspinatus, teres minor, subscapularis)
-
Joint capsule and ligaments
When these are disrupted by trauma (e.g., a fall on an outstretched hand), dislocation may ensue.
Radiographic Signs of Anterior Shoulder Dislocation on CXR
 |
| Figure 2. Another example of anterior shoulder dislocation on CXR |
Though chest radiographs are suboptimal for dedicated shoulder evaluation, certain key findings can reveal dislocation:
-
Loss of articulation between the humeral head and the glenoid
-
Medial and inferior displacement of the humeral head relative to the glenoid
-
Empty glenoid sign
-
A coexisting fracture may sometimes be visible (e.g., greater tuberosity)
These features are readily appreciated in Figure 1 and Figure 2, indicating anterior glenohumeral dislocation.
Clinical Context and Importance of Chest X-ray
Chest X-rays are frequently obtained in:
-
Polytrauma settings
-
Postoperative shoulder or thoracic procedures
-
Evaluation of chest pain, dyspnea, or rib trauma
In such cases, a shoulder dislocation may go unrecognized unless deliberately reviewed.
Pearl: Always trace the humeral head to assess its alignment with the glenoid, even on CXRs.
Differential Diagnosis
When evaluating glenohumeral misalignment, consider:
-
Posterior dislocation (rare): Often due to seizures, electrocution; the humeral head appears fixed in internal rotation (lightbulb sign)
-
Fracture-dislocation
-
Proximal humeral fracture
-
Normal variant (e.g., external rotation)
Management Overview
Anterior shoulder dislocations are typically treated with closed reduction under sedation, followed by:
-
Neurovascular assessment
-
Immobilization (sling)
-
Follow-up orthopedic evaluation
-
MRI (if labral or rotator cuff injury suspected)
Surgical intervention is rare but considered in recurrent dislocations or associated soft tissue damage.
Quiz
1. What radiologic sign in Figure 1 is the most suggestive of anterior glenohumeral dislocation?
A) The humeral head overlaps the glenoid
B) The humeral head is displaced medially and inferiorly
C) The humeral head appears rounded and centered
D) Presence of pneumothorax
2. Which structure provides the greatest dynamic stability to the glenohumeral joint?
A) Glenoid labrum
B) Joint capsule
C) Rotator cuff muscles
D) Coracoacromial ligament
3. A 55-year-old man presents after a fall. CXR shows an inferiorly displaced humeral head. What is the most likely diagnosis?
A) Posterior shoulder dislocation
B) Normal shoulder alignment
C) Anterior shoulder dislocation
D) Acromioclavicular joint separation
Answer & Explanation
1. Answer: B), Explanation: The humeral head in anterior dislocation typically lies medial and inferior to the glenoid fossa on AP chest views. This is a hallmark of anterior displacement.
2. Answer: C), Explanation: The rotator cuff dynamically stabilizes the humeral head within the glenoid through active muscular control during movement.
3. Answer: C), Explanation: Inferomedial displacement on CXR strongly suggests anterior glenohumeral dislocation, particularly following trauma.
Discussion: Why It Matters
Missed shoulder dislocations on CXR can delay diagnosis and worsen outcomes. Radiologists and emergency physicians should maintain a high index of suspicion, particularly when the shoulder contour appears asymmetric or if the patient has shoulder pain post-trauma.
Chest radiographs offer a unique opportunity to detect dislocations incidentally and must not be limited to pulmonary or cardiac assessment alone.
Conclusion
This review underscores the importance of evaluating the shoulder joint on chest radiographs, especially in trauma cases. Anterior glenohumeral dislocation, the most common type, can often be visualized on routine chest X-rays if actively sought. Proper interpretation leads to faster intervention and better patient outcomes.
References
[1] A. M. Dilley, S. A. Funk, “Radiographic Evaluation of Shoulder Dislocations,” AJR Am J Roentgenol, vol. 189, no. 2, pp. 367–373, 2007.
[2] R. W. Stoller, Magnetic Resonance Imaging in Orthopaedics and Sports Medicine, 3rd ed., Lippincott Williams & Wilkins, 2007.
[3] A. L. Kassarjian et al., “Imaging of Shoulder Trauma,” Radiol Clin North Am, vol. 40, no. 2, pp. 263–277, Mar. 2002.
[4] J. F. Gielen et al., “MR Imaging of Rotator Cuff Disorders,” Eur J Radiol, vol. 65, no. 1, pp. 8–17, Jan. 2008.
[5] R. Mall et al., “Incidence and Outcomes of Shoulder Dislocations,” J Bone Joint Surg Am, vol. 84, pp. 403–409, 2002.
[6] C. M. Robinson et al., “Recurrent Shoulder Dislocation,” J Bone Joint Surg Br, vol. 84, no. 5, pp. 679–685, Jul. 2002.
[7] D. M. Tennent, A. J. Pearse, “Management of Traumatic Anterior Shoulder Dislocation,” BMJ, vol. 332, no. 7543, pp. 1124–1128, 2006.



Comments
Post a Comment