Pediatric Cerebral Palsy (CP)
Pediatric Cerebral Palsy (CP)
1. Cause and Etiology
Cerebral Palsy (CP) is a group of permanent,
non-progressive neurological disorders caused by abnormal brain
development or damage to the developing brain. These disorders lead to motor
dysfunction and are often associated with impairments.
Etiology
CP can arise from multiple etiological factors, which are broadly
classified into:
a) Prenatal Causes (~70–80% of cases)
- Periventricular
leukomalacia (PVL): White
matter injury due to hypoxia-ischemia.
- Congenital
brain malformations:
Lissencephaly, polymicrogyria, etc.
- Intrauterine
infections: Cytomegalovirus,
toxoplasmosis, rubella.
- Maternal risk
factors: Preeclampsia, diabetes,
thyroid dysfunction, substance use.
b) Perinatal Causes
- Birth
asphyxia/hypoxic-ischemic encephalopathy (HIE)
- Preterm birth (especially <32 weeks of gestation)
- Low birth
weight (<2,500 g)
- Neonatal
stroke
- Prolonged
labor or abnormal presentation
c) Postnatal Causes
- Severe
neonatal jaundice (kernicterus)
- Traumatic brain
injury
- CNS
infections (e.g., meningitis, encephalitis)
- Seizures or
metabolic disorders in infancy
Most cases of CP are due to events before or around birth, rather
than later acquired insults.
2. Pathophysiology
CP results from non-progressive brain injury or abnormal
development that impairs motor control centers, particularly within:
- Cerebral
cortex
- Basal ganglia
- Cerebellum
- Periventricular
white matter
Major Pathological Mechanisms:
- Ischemic/hypoxic
injury: Especially in preterm
infants.
- Inflammation
and oxidative stress are triggered by maternal infections or neonatal complications.
- Abnormal
neuronal migration or proliferation during fetal development.
These events cause disruption of corticospinal tract development,
leading to:
- Muscle tone abnormalities
(spasticity, hypotonia)
- Impaired motor
coordination and control
- Abnormal reflex patterns
3. Epidemiology
|
Parameter |
Value |
|
Global prevalence |
~2 to 3 per 1,000 live births |
|
Higher in preterm infants |
~40–100 per 1,000 very low birth weight (VLBW) infants |
|
Male-to-female ratio |
~1.3:1 |
|
Incidence in high-income countries |
~1.5–2 per 1,000 live births |
|
Incidence in low-resource settings |
Higher due to limited prenatal care |
4. Clinical Presentation
The clinical picture varies significantly depending on the type, severity,
and distribution of brain injury.
Motor Symptoms (Core Features):
- Abnormal
muscle tone: Spasticity (↑ tone),
hypotonia (↓ tone)
- Delayed motor
milestones
- Abnormal
postures and reflexes
- Movement
disorders: Dystonia, chorea,
athetosis, ataxia
Associated Impairments (common in moderate to severe
cases):
- Intellectual
disability (~30–50%)
- Speech and
language disorders
- Seizures (~25–45%)
- Hearing or
vision impairment
- Feeding/swallowing
difficulties
- Behavioral
and emotional disorders
5. Classification of CP
By Movement Type:
|
Type |
Features |
|
Spastic CP |
Most common (~70–80%); stiff, jerky movements |
|
Dyskinetic CP |
Involuntary movements (dystonia, choreoathetosis) |
|
Ataxic CP |
Poor balance and coordination |
|
Mixed CP |
Combination of types (e.g., spastic + dyskinetic) |
By Topography:
- Hemiplegia: One side of the body affected
- Diplegia: Mainly lower limbs
- Quadriplegia: All four limbs involved
6. Imaging Features
Neuroimaging is essential for diagnosis, particularly in unclear cases or
when determining etiology.
MRI (preferred modality):
- Periventricular
leukomalacia (PVL): Seen in
preterm infants; indicates white matter damage.
- Cerebral
atrophy
- Delayed
myelination
- Basal ganglia
injury: Especially in term
infants with HIE.
- Congenital
malformations: e.g.,
schizencephaly, lissencephaly.
CT Scan:

- May detect calcifications
or hemorrhages, but is less sensitive than MRI for white matter injury.
MRI findings correlate with motor and cognitive outcomes.
7. Treatment and Management
There is no cure for CP, but early, multidisciplinary intervention
significantly improves outcomes.
Multimodal Approach:
- Physical
therapy – Improves strength,
flexibility, and motor skills.
- Occupational
therapy – Enhances functional
independence (e.g., dressing, feeding).
- Speech and
language therapy – For
communication and feeding/swallowing difficulties.
- Orthopedic
interventions – For joint
contractures, scoliosis, hip dislocations.
- Pharmacotherapy:
- Oral medications: Baclofen, diazepam, tizanidine for spasticity
- Botulinum
toxin injections: For focal
muscle overactivity
- Antiepileptics: If seizures are present
- Surgical
options:
- Selective
dorsal rhizotomy (SDR) for severe
spasticity
- Orthopedic
surgeries: Tendon lengthening,
osteotomy
- Assistive
technologies:
- Wheelchairs, walkers,
communication devices
- Educational
and psychosocial support:
- Inclusive education,
behavioral therapy, and caregiver support
8. Prognosis
The outcome depends on type, severity, comorbidities,
and timeliness of intervention.
Favorable Prognostic Indicators:
- Milder motor involvement
- No intellectual
disability
- Ambulation by age 2
Less Favorable:
- Severe spastic
quadriplegia
- Severe intellectual
disability
- Persistent epilepsy
Life Expectancy:
- Normal or near-normal in
mild CP
- Reduced in severe CP with
multiple comorbidities
✅ Early intervention, family education, and comprehensive care can
drastically improve functional independence and quality of life.
Summary Table
|
Category |
Details |
|
Cause |
Prenatal/perinatal/postnatal brain injury or abnormal development |
|
Pathophysiology |
Non-progressive injury affecting motor control centers |
|
Epidemiology |
2–3/1,000 live births; higher in preterm infants |
|
Symptoms |
Spasticity, delayed milestones, abnormal movement, and associated
impairments |
|
Imaging |
MRI shows PVL, atrophy, basal ganglia lesions, and malformations |
|
Treatment |
Multidisciplinary rehab, medication for spasticity, and surgery for
deformities |
|
Prognosis |
Highly variable; better with early therapy and mild forms |
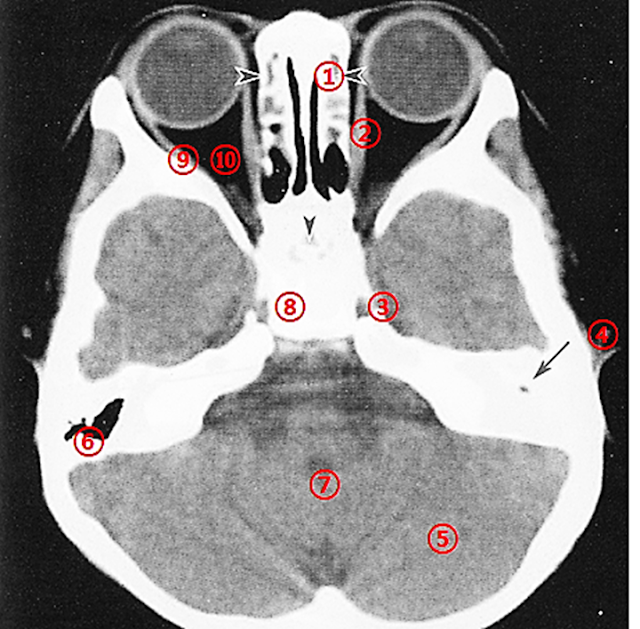
Axial CT Slice Through the
Central Orbit
Normal Image
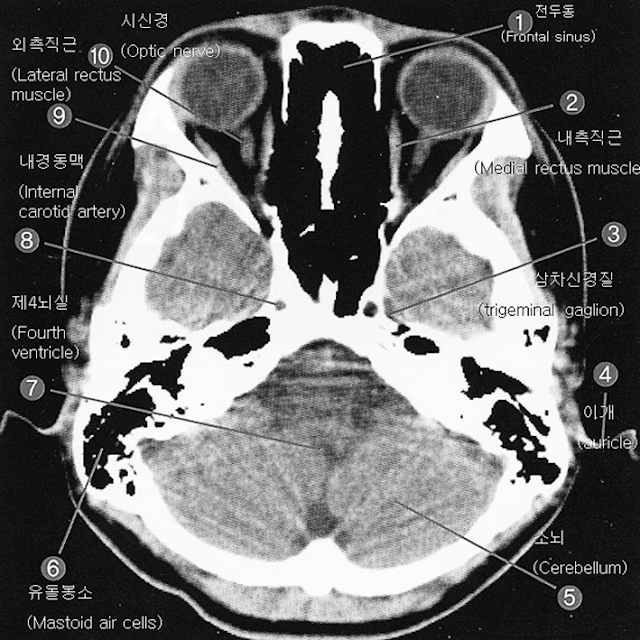
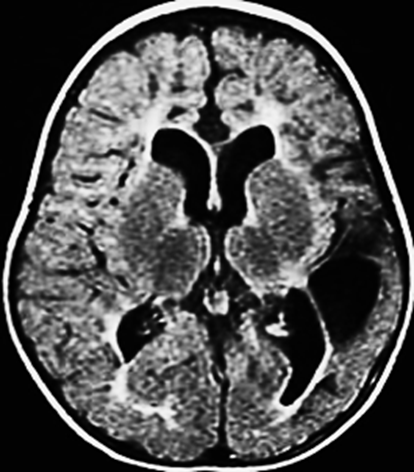
Image of a 4-Year-Old Male with Developmental Delay

Findings:
 Underdevelopment of the left mastoid air cells
(Lt mastoid air cell) is observed,
and the mastoid antrum shows soft tissue density rather than air.
Underdevelopment of the left mastoid air cells
(Lt mastoid air cell) is observed,
and the mastoid antrum shows soft tissue density rather than air.- These findings are suspicious
for chronic otitis media.
- The sphenoethmoidal sinus is undeveloped.
- A white appearance of the
mastoid air cells on CT can be due either to poor development
(chronic otitis media) or retention of fluid or secretions (acute
otitis media).
- Bone window
settings—achieved by increasing
the window width and raising the window level—are useful for
distinguishing between these two scenarios.
Advantages of CT Bone Settings:
Compared to traditional bone imaging techniques, CT bone window settings
offer the following advantages:
- Precision: CT provides detailed visualization of bony
structures, enabling accurate planning and execution of realignment
procedures.
- Customization: Virtual reconstruction allows for treatment
plans tailored to each patient’s unique anatomy and injury pattern.
- Minimally
Invasive: In some cases,
CT-guided bone procedures allow for less invasive interventions,
resulting in shorter recovery times and reduced risk of
complications.
CT Terms: Window Level (WL) and Window Width (WW)
These terms refer to image processing parameters used in CT to optimize
the visibility of specific tissues or structures in the scanned area.
Window Level (WL):
- Determines the center
value of the gray scale range displayed in the image.
- Controls image
brightness: increasing WL makes the image brighter, decreasing WL makes it darker.
- It’s adjusted to
highlight specific tissues:
- Higher WL for bone
- Lower WL for soft
tissues
Window Width (WW):
- Determines the range
of CT values (in Hounsfield units) displayed as shades of gray.
- Controls image
contrast:
- Wider WW = greater contrast (better distinction
between different tissues)
- Narrower WW = less contrast, but better
visualization of subtle differences in similar-density tissues
For example:
- A wide WW enhances
contrast between bone and soft tissue
- A narrow WW is
better for distinguishing subtle soft tissue density variations
Discussion: Pediatric Cerebral Palsy (CP)
Cerebral Palsy (CP) is a movement
and muscle control disorder caused by brain injury that occurs at
birth or during early infancy.
Due to abnormal brain development or brain injury, children
with CP may experience difficulties with:
- Postural control
- Muscle tone regulation
- Balance
- Voluntary movement
Causes of CP:
1. Prenatal or Perinatal Brain Injury:
- Damage may occur in the fetal
period or during childbirth.
- Causes include trauma,
oxygen deprivation, or stimulation-related injury.
2. Postnatal Brain Injury:
- Injury after birth from trauma,
infection, or illness may disrupt normal brain development and
function, increasing the risk of CP.
Symptoms of CP-Related Motor Impairment:
- Spasticity (muscle stiffness)
- Reduced
muscle strength
- Postural
instability
- Impaired
coordination
- Gait
abnormalities
- Fine motor
difficulties (e.g., hand use issues)
These motor impairments can affect daily life and functional
independence.
Management and Rehabilitation:
Although CP has no cure, comprehensive therapy can significantly
improve function:
- Physical
therapy
- Occupational
therapy
- Speech therapy
- Use of assistive
devices
Each treatment plan should be personalized to the patient's condition and needs.



Comments
Post a Comment